
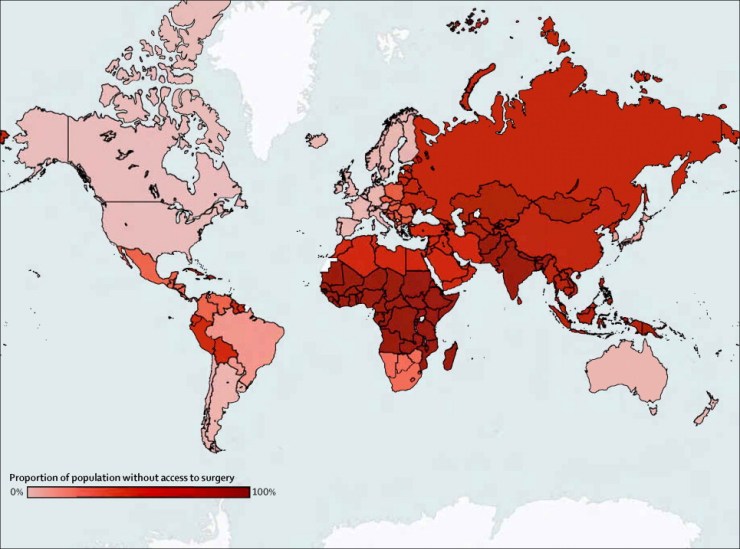
Five billion people –five out of every seven people in the world- do not have timely access to safe surgical care when needed. Lack of surgical, anaesthesia, and obstetric care is responsible for approximately 18 million preventable deaths every year, over four times the mortality due to HIV, tuberculosis, and malaria combined. Besides high mortality rates, surgically treatable conditions make up 28-32% of the global burden of disease, ranging from congenital malformations to obstetric complications, from malignancies to cardiovascular disease, and from road traffic injuries to violence. Every year, 313 million operations take place around the world, yet only 6.5% takes place in the poorest third of the world, representing the people that need surgical care the most. As a result, by 2030, 2.28 million additional surgeons, anaesthesiologists and obstetricians are needed to provide the additional 143 million procedures needed per year. To support this and scale up surgical care globally, an investment of ‘only’ $350 billion is required, preventing a potential loss of $12.3 trillion in economic growth by LMICs by 2030.
History
In 1980, former Director-General of the World Health Organization (WHO) Dr. Halfdan Mahler brought disparities in access to and quality of surgical care to the attention of the world in his address “Surgery and Health for All” to the 12th biennial World Congress of the International College of Surgeons: “The vast majority of the world’s population has no access whatsoever to skilled surgical care and little is being done to find a solution. I beg of you to give serious consideration to this most serious manifestation of social inequity in health care”. Unfortunately, this moral call for action did not bring the needed paradigm shift, with surgery consistently being considered as too expensive and too complex to scale up on a global level.
In 2008, Paul Farmer (Harvard Medical School; Partners in Health) and Jim Y. Kim (Harvard Medical School; current (12th) President of the World Bank Group) published a non-surgical view of “global surgery” with their paper “Surgery and Global Health: A View Beyond the OR”.2 The paper coined surgery as “the neglected stepchild of global health”, calling for increased attention and awareness of surgeons and policymakers about surgery as a vital component of global health.
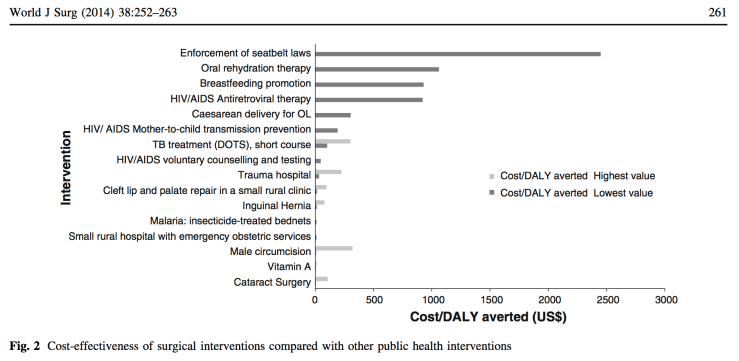
In 2014, Caris E. Grimes et al. published “Cost-effectiveness of Surgery in Low- and Middle- income countries: A Systematic Review” in the World Journal of Surgery.3 The review proved the favourable cost-effectiveness (dollars spent per DALY averted) of basic surgery in low- resource settings compared to other public health interventions, such as oral rehydration therapy, breast feeding promotion and anti-retroviral therapy for HIV. This led to the conclusion that simple surgical interventions, both life-saving and disability-preventing, should be integrated in public health policies and be accessible at district hospitals, further debunking the previous myth of the relative high costs of surgical care.
2015 proved to be a pivotal year for global surgery. The Lancet Commission on Global Surgery (LCoGS) mapped the global state of access to surgical and anaesthesia care, which they published in their report “Global Surgery 2030: evidence and solutions for achieving health, welfare and economic development.”, providing the international community with the needed rationale for addressing global surgical care.1 Moreover, the WHO and its member states acknowledged the importance of addressing the global state of surgical systems to promote better health, well-being and economic growth. During the 68th World Health Assembly, the resolution WHA68.15 “Strengthening Emergency and Essential Surgical and Anaesthesia Care as a Component of Universal Health Coverage” was adopted, putting the surgical foot in the global health door. To bring this memorable point in time to the attention of social media, InciSioN – International Student Surgical Network started Global Surgery Day on May, 25th 2015, which has continued and increased in the years to come.
In 2017, the 70th WHA marked another big step towards achieving safe surgical care for all, with multiple stakeholders (WHO, Member States, and civil society, including NGOs and academic institutions) further drawing the attention to global surgery. Zambia was the first country to announce their National Surgical, Obstetric and Anaesthesia Plan (NSOAP) –a framework for integrating surgical care in a country’s health agenda- which was incorporated in Zambia’s National Health Strategic Plan for 2017-2021. Realizing that health systems strengthening cannot take place without addressing surgical systems, other countries are following, being in the process of developing their NSOAP or inspired to start the process for their country.
This introduction was first published in “Global Surgery: An Introduction” by Dominique Vervoort and recreated with permission.
References:
- Meara JG, Leather AJM, Hagander L, et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569-624. doi:10.1016/S0140-6736(15)60160-X.
- Farmer PE, Kim JY. Surgery and global health: A view from beyond the OR. World J Surg. 2008;32(4):533-536. doi:10.1007/s00268-008-9525-9.
- Grimes CE, Henry JA, Maraka J, Mkandawire NC, Cotton M. Cost-effectiveness of surgery in low- and middle-income countries: A systematic review. World J Surg. 2014;38(1):252-263. doi:10.1007/s00268-013-2243-y.
- Alkire BC, Raykar NP, Shrime MG, et al. Global access to surgical care: A modelling study. Lancet Glob Heal. 2015;3(6):e316-e323. doi:10.1016/S2214-109X(15)70115-4.
