
Global health has long been dominated by communicable (infectious) diseases and maternal and child primary care. Appropriately so, although arguably out of proportion relative to, for example, non-communicable diseases, including cardiovascular diseases, and trauma given the burden of disease. Since 2015, the field of global surgery has made great strides due to an increased understanding of the gaps therein and the importance thereof in low- and middle-income countries (LMICs). To date, however, cardiac surgery is rarely touched upon – many a time due to pre-existing myths.
.
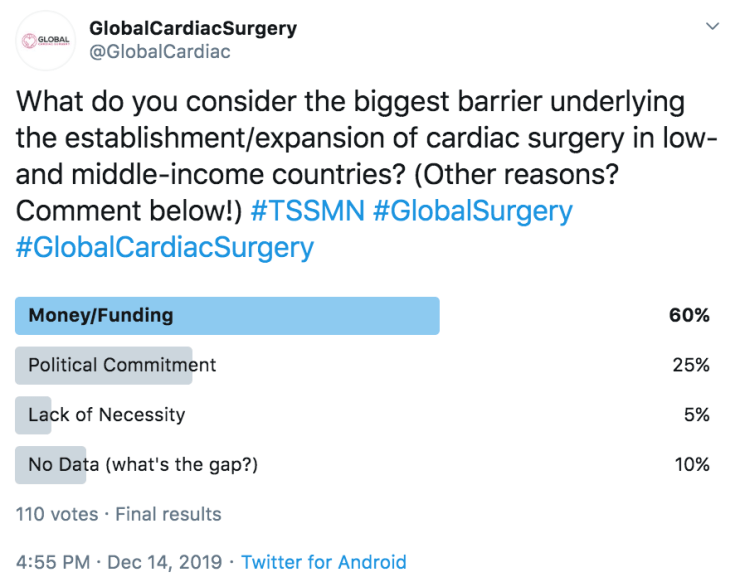
On Twitter, @GlobalCardiac polled its followers to assess what they assumed are the biggest barriers underlying the establishment and expansion of cardiac surgical services in LMICs. The options, a non-exhaustive list, included funding, political commitment, a lack of necessity, and a lack of data, as well as a free comment section. Among 110 voters in 48 hours, the results were clear:
.
.
Overall, 60% (n = 66) of respondents considered that money/funding (or better, a lack thereof) posed the biggest barrier. With good reason, as cardiac surgery involves a large continuum of services pre-operatively (e.g., imaging), intra-operatively (e.g., heart-lung machine), and post-operatively (e.g., intensive care). In addition to the center’s upfront costs to provide these services, operational costs commonly fall upon the patient or sponsor in LMICs. Cardiac surgeries have a wide range of costs between and within countries but commonly pass the $10,000 mark. In India ($1,500) and Vietnam ($2,000-$5,000), the costs of coronary artery bypass grafting have significantly been reduced through local procurement and economies of scale, which is, however, still an exception in LMICs.
.
25% (n = 28) assumed that political commitment was the strongest driver (conversely, a lack thereof the biggest barrier) towards the scaling of cardiac surgical care in LMICs. Cardiac surgery is often considered a “trophy” for a given hospital or health system, whereby simply having the service, regardless of volume or accessibility, is touted as a “win” for the country. However, politicians also understand the dynamics of domestic elections: if one wants to be re-elected, proof of impact is needed; establishing and expanding cardiac surgical services may take a longer timeline than the average governmental term due to training cardiac teams and the long learning curve for hospitals. Meanwhile, @VictorDayan1 and @bzheleva argued that funding and political commitment go hand-in-hand based on countries’ priorities and donors’ earmarking:
.
.
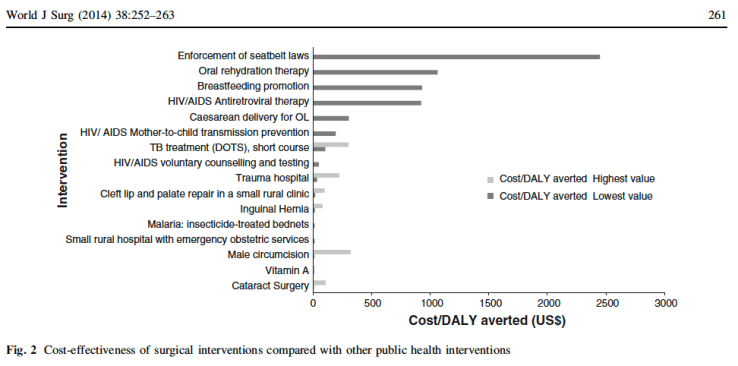
One in ten (n = 11) considered a lack of available data to better understand the pre-existing gaps major impediments in the ability to adequately advocate for expansion of said services to policymakers and funders. Understandably so, as a large scarcity of data exists in global cardiac surgery due to a lack of standardized databases, many of which are overlapping in high-income countries but including few LMICs. Moreover, countries do not actively collect surgical indicators and a gross lack of cardiac surgeons in LMICs prevents uniform accreditation and reporting. As highlighted by @hibazghandour, “we urgently need more knowledge of what is going on [and] then we can focus on diplomatically improving political commitment”. A minority (n = 5) replied that there is a lack of necessity for cardiac surgical services in LMICs. The role thereof in LMICs, especially in low-income countries, remains debatable, with some arguing for scaling of models whereby patients are solely sent abroad, although new cost-effectiveness data hints at the feasibility and utility of cardiac surgery in LMICs.
.
Lastly, several individuals raised important considerations beyond the available options. Of note, the role of professional societies was raised by @DVervoort94 to take the lead in addressing pre-existing gaps through data collection, industry empowerment, and ethical and sustainable capacity-building. Meanwhile, the Cardiac Surgery Intersociety Alliance, a collaborative by the major regional cardiac surgery societies across different continents and the World Heart Federation, has taken the first step of leveraging additional funding for existing low-volume cardiac centers in LMICs in order to better equip these facilities and, in turn, increase patient volume.
.
.
Additionally, workforce issues were common themes across different open responses. These appeals were raised by @RwandaCardiac in Rwanda (which recently welcomed its first own cardiac surgeon), @ElhadiMuhammed in Libya (7 cardiac surgeons for 6.4 million people), and @jwlartigue in Haiti (no cardiac surgeon for 11 million people), emphasizing the large gaps in the availability of adult and pediatric cardiac surgeons in LMICs across the globe.
.
Although funding and political commitment clearly outweigh other factors when considering cardiac surgery in LMICs, it is clear that the subject is a multi-disciplinary and multi-sectoral issue. Advancing cardiac care in LMICs is a complex process affecting the entire health system and thus requiring a multi-pronged approach. A better understanding of the existing gaps in the provision of cardiac services and increasing relevant high-level advocacy will ultimately be required to catalyze monetary and political change.
 Ernest Simpunga (second from right): “Surgery in India would cost 15,000 dollars, which we could not afford, and it would take three years for visiting teams to treat me. Seeing cardiologists and taking medicines costed hundreds of dollars per month, so I had to change to a cheaper high school.“
Ernest Simpunga (second from right): “Surgery in India would cost 15,000 dollars, which we could not afford, and it would take three years for visiting teams to treat me. Seeing cardiologists and taking medicines costed hundreds of dollars per month, so I had to change to a cheaper high school.“ Dr. Koiral (third from left): “Highly specialized, but widely needed care such as cardiac surgery can efficiently be provided in low- and middle-income countries with effective care models. In Nepal, we treat patients from neighbouring countries due to our low costs for cardiac surgery.“
Dr. Koiral (third from left): “Highly specialized, but widely needed care such as cardiac surgery can efficiently be provided in low- and middle-income countries with effective care models. In Nepal, we treat patients from neighbouring countries due to our low costs for cardiac surgery.“
